Trisomy 18 (Edwards Syndrome)
Trisomy 18, also known as Edwards syndrome, is a congenital genetic disorder caused by a chromosomal abnormality.
It was named after John H. Edwards, a British geneticist who first described and reported it in 1960.
The incidence of Trisomy 18 is approximately 1 in 3,500 to 8,500 live births, and it is a chromosomal abnormality that is more common in females (female-to-male ratio of 3:1).*1
It was named after John H. Edwards, a British geneticist who first described and reported it in 1960.
The incidence of Trisomy 18 is approximately 1 in 3,500 to 8,500 live births, and it is a chromosomal abnormality that is more common in females (female-to-male ratio of 3:1).*1
\ Understand the risk of Edwards syndrome in your baby /
Causes
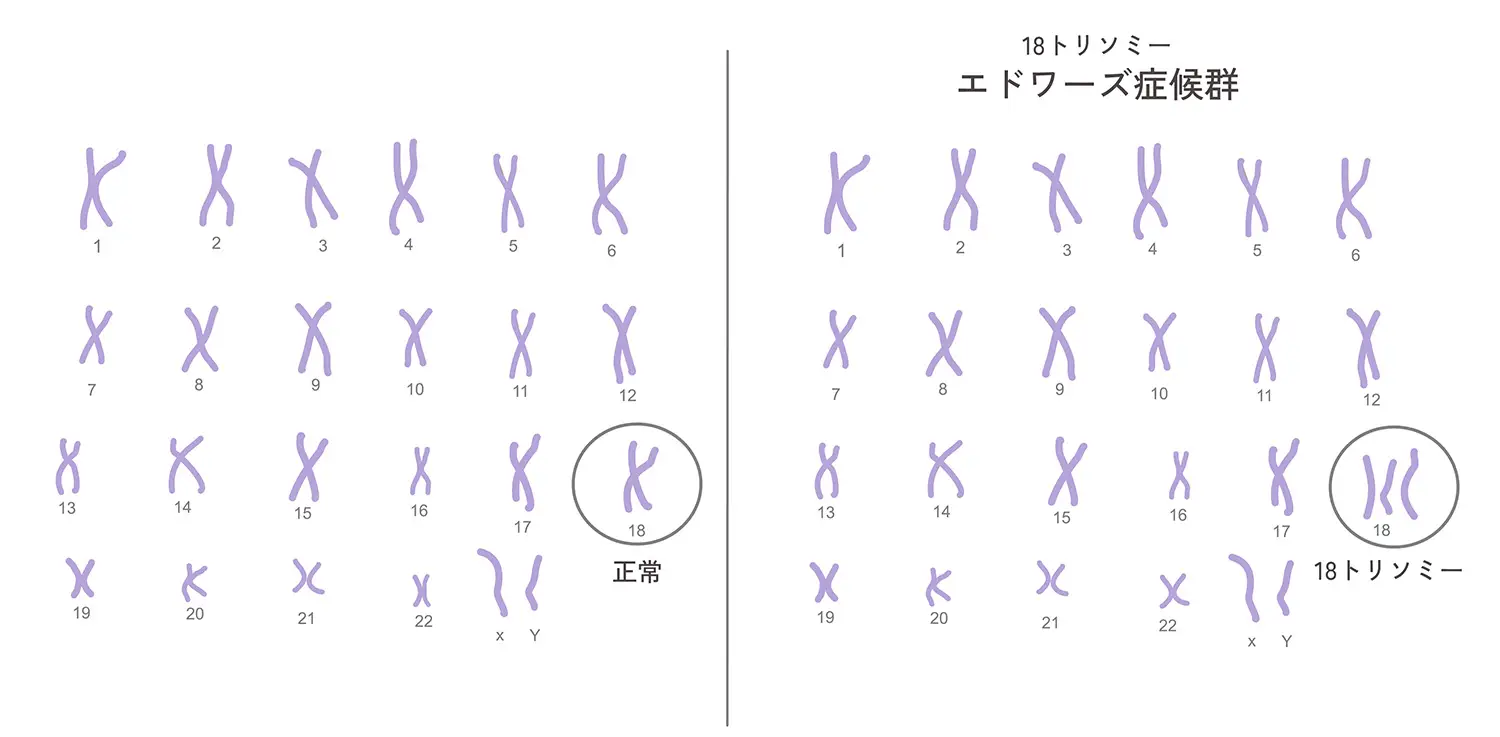
Edwards syndrome (Trisomy 18) occurs when there are three copies of chromosome 18 in cells instead of the usual two.
This chromosomal abnormality can occur due to several mechanisms:*2
<Standard Trisomy 18>
During the formation of parental reproductive cells (egg or sperm), chromosomes fail to separate correctly (nondisjunction). As a result, an extra chromosome 18 is included in the child's cells, leading to three copies of chromosome 18 in the fertilized egg. This nondisjunction accounts for more than 90% of Trisomy 18 cases.
<Mosaic Trisomy 18>
Nondisjunction occurs during early cell divisions after fertilization. Consequently, the extra chromosome 18 exists in only a portion of the body's cells. In this case, symptoms may be milder than in standard Edwards syndrome. Mosaicism accounts for about 5% of Trisomy 18 cases.
<Translocation Trisomy 18>
This occurs when a portion of chromosome 18 becomes attached (translocated) to another chromosome. If either parent carries a translocated chromosome, Trisomy 18 can be inherited. Translocation accounts for about 2% of Trisomy 18 cases.
Since the primary cause of Edwards syndrome is a random chromosomal event occurring during the formation of parental reproductive cells, prevention is generally difficult. While the risk increases with maternal age, it can also occur in children born to younger parents.
This chromosomal abnormality can occur due to several mechanisms:*2
<Standard Trisomy 18>
During the formation of parental reproductive cells (egg or sperm), chromosomes fail to separate correctly (nondisjunction). As a result, an extra chromosome 18 is included in the child's cells, leading to three copies of chromosome 18 in the fertilized egg. This nondisjunction accounts for more than 90% of Trisomy 18 cases.
<Mosaic Trisomy 18>
Nondisjunction occurs during early cell divisions after fertilization. Consequently, the extra chromosome 18 exists in only a portion of the body's cells. In this case, symptoms may be milder than in standard Edwards syndrome. Mosaicism accounts for about 5% of Trisomy 18 cases.
<Translocation Trisomy 18>
This occurs when a portion of chromosome 18 becomes attached (translocated) to another chromosome. If either parent carries a translocated chromosome, Trisomy 18 can be inherited. Translocation accounts for about 2% of Trisomy 18 cases.
Since the primary cause of Edwards syndrome is a random chromosomal event occurring during the formation of parental reproductive cells, prevention is generally difficult. While the risk increases with maternal age, it can also occur in children born to younger parents.
Symptoms
Trisomy 18 (Edwards Syndrome) causes various symptoms affecting development, internal organs, and physical features:*3
<Physical Characteristics>
• Low birth weight and slow growth
• Microcephaly (small head) and abnormal head shape
• Ocular abnormalities, strabismus, etc.
• Small lower jaw (micrognathia)
<Cognitive and Developmental Issues>
• Severe intellectual disability
• Significant developmental delays
<Medical Problems>
• Congenital heart defects
• Respiratory disorders
• Gastrointestinal anomalies
• Hearing impairment
Many infants with Edwards syndrome face life-threatening medical issues shortly after birth, resulting in a low survival rate. However, depending on the severity and specific symptoms, some children can survive for a longer period.
<Physical Characteristics>
• Low birth weight and slow growth
• Microcephaly (small head) and abnormal head shape
• Ocular abnormalities, strabismus, etc.
• Small lower jaw (micrognathia)
<Cognitive and Developmental Issues>
• Severe intellectual disability
• Significant developmental delays
<Medical Problems>
• Congenital heart defects
• Respiratory disorders
• Gastrointestinal anomalies
• Hearing impairment
Many infants with Edwards syndrome face life-threatening medical issues shortly after birth, resulting in a low survival rate. However, depending on the severity and specific symptoms, some children can survive for a longer period.
Treatments
While there is no cure for Edwards syndrome, medical care and therapeutic support are provided to address specific symptoms and complications.*4
Recently, life expectancy has improved in some cases due to advances in neonatal intensive care and cardiac surgery.
<Neonatal Intensive Care>
Infants receive 24-hour monitoring of heart rate, respiration rate, blood oxygen levels, and blood pressure. Various treatments, including mechanical ventilation, medications, and intravenous fluids, are administered based on the child's condition.
It is essential to plan comprehensive medical care, developmental support, and family counseling tailored to the child's needs.
Recently, life expectancy has improved in some cases due to advances in neonatal intensive care and cardiac surgery.
<Neonatal Intensive Care>
Infants receive 24-hour monitoring of heart rate, respiration rate, blood oxygen levels, and blood pressure. Various treatments, including mechanical ventilation, medications, and intravenous fluids, are administered based on the child's condition.
It is essential to plan comprehensive medical care, developmental support, and family counseling tailored to the child's needs.
References
- (1) American Journal of Obstetrics and Gynecology, "Prevalence and epidemiological data of Trisomy 18" / 2004
- (2) SSM Health Cardinal Glennon Children's Hospital, "Causes and classification of Trisomy 18 (Edwards Syndrome)"
- (3) MedlinePlus (U.S. National Library of Medicine), "Symptoms and genetic information of Trisomy 18"
- (4) National Health Service UK, "Diagnosis and treatment of Edwards' syndrome (trisomy 18)"
- (5) Ministry of Health, Labour and Welfare, "Report on Information Provision Regarding Prenatal Testing such as NIPT" / 2023
Frequently Asked Questions
Q.What is Trisomy 18 (Edwards Syndrome)?
A.
Trisomy 18 (Edwards syndrome) is a congenital disorder caused by the presence of three copies of chromosome 18 instead of the usual two. It was first described by British geneticist John H. Edwards. The incidence is approximately 1 in 3,500 to 8,500 live births, occurring more frequently in females (female-to-male ratio of 3:1).
Q.What causes Trisomy 18?
A.
There are three main causes: Standard type (over 90% of cases) is caused by chromosomal nondisjunction during the formation of germ cells. Mosaic type (about 5%) is caused by nondisjunction during early cell divisions after fertilization, resulting in an extra chromosome 18 in only a portion of body cells. Translocation type (about 2%) occurs when a part of chromosome 18 attaches to another chromosome (2). Advanced maternal age is a risk factor, but it can also occur in children of younger parents.
Q.What are the main symptoms of Trisomy 18?
A.
Symptoms are broadly classified into three categories: Physical features include low birth weight, microcephaly, and a small lower jaw. Cognitive and developmental issues include severe intellectual disability and developmental delays. Medical problems include congenital heart defects, respiratory disorders, gastrointestinal anomalies, and hearing impairment (3).
Q.Is there a treatment for Trisomy 18?
A.
There is currently no cure for Trisomy 18. Treatment consists of medical management and therapeutic support tailored to the specific symptoms. Neonatal intensive care includes 24-hour monitoring of heart rate, breathing, oxygen levels, and blood pressure, along with mechanical ventilation, medications, and intravenous fluids. In recent years, prognosis has improved in some cases due to neonatal intensive care and cardiac surgery (4).
Q.Is there a way to screen for Trisomy 18 risk before birth?
A.
Yes, Non-Invasive Prenatal Testing (NIPT) allows screening for fetal Trisomy 18 risk during pregnancy. NIPT is a non-invasive test that analyzes fetal DNA fragments in the mother's blood. Since it only requires a blood draw, it poses no direct risk to the fetus. seeDNA provides high-precision NIPT screening (5).