Condition Detected by NIPT Part 5: Klinefelter Syndrome
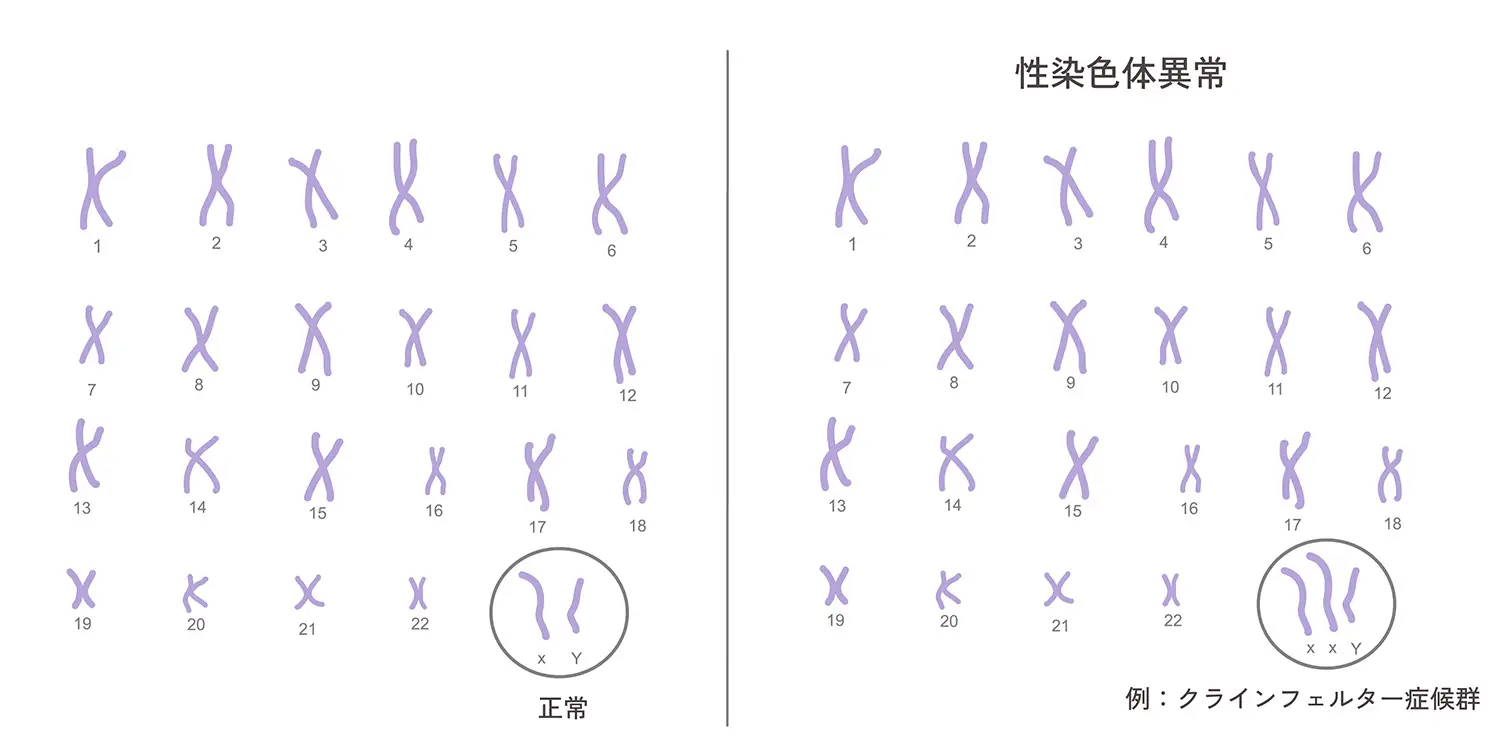
Klinefelter syndrome is a condition in which males develop clinical symptoms such as testicular hypoplasia and gynecomastia. It was first described by Klinefelter in 1942, and its cause was identified as a sex chromosome abnormality in 1959. The karyotype is 47, XXY, representing a sex chromosome abnormality with one or more extra X chromosomes. Klinefelter syndrome occurs relatively frequently, at a rate of 1 in 1,000 males. ※1 It is one of the most common causes of male hypogonadism.
Find out the risk of Klinefelter syndrome in the fetus
Cause
The cause of Klinefelter syndrome is a sex chromosome abnormality with a 47, XXY karyotype. The 47, XXY karyotype is classified into two types depending on the presence of mosaicism. ※2
80% to 85% of individuals with Klinefelter syndrome have the 47, XXY karyotype. The cause is nondisjunction of sex chromosomes during meiosis of parental germ cells. Cases inherited from the mother are slightly more common at 56% compared to those from the father.
The remaining approximately 15% have various mosaic types such as 46, XY/47, XXY, 46, XX/47, XXY, 46, XX/46, XY/47, XXY, and 46, XY/48, XXXY. Because some cells in the body have a normal karyotype, clinical findings are often milder than in the non-mosaic type.
Symptoms
Symptoms of Klinefelter syndrome appear in areas such as intelligence, growth, and gonadal function. ※3
Intelligence
The average IQ of individuals with Klinefelter syndrome is often around 85 to 90, which is slightly lower than the general average, but severe intellectual disability is rarely observed. While there is often no major obstacle in daily life, weaknesses tend to be noticeable in abilities related to language (speaking, listening, reading, writing). For example, comprehension of words may be slow, or it may be difficult to express ideas in writing or conversation. Consequently, individuals often struggle in subjects such as national language or English, and learning may take more time.
Growth
Individuals with Klinefelter syndrome tend to be tall. In particular, they often have long arms and legs and an overall long, slender build. This is because bone growth continues longer due to low levels of the male hormone testosterone during growth. As a result, they may grow taller than typical males, and it is said that many reach 180 cm or taller. However, since there are individual differences, not everyone with Klinefelter syndrome will have tall stature.
Hypogonadism
In many cases, the testes and scrotum are confirmed to be slightly small, and almost all patients are infertile. Approximately 30% of individuals show breast enlargement known as "gynecomastia." In rare cases, abnormalities in the elbow joint, malformation of the genitalia, curvature of the spine (scoliosis), osteoporosis, diabetes, breast tumors, and germ cell tumors may appear.
Explanation and Diagnosis Method ※4
Klinefelter syndrome is a disease that is often diagnosed based on physical changes observed after puberty. Diagnosis involves performing genetic testing on cells to examine the condition of sperm chromosomes (whether they are the 47, XXY type). In addition, blood tests to measure hormone levels frequently reveal elevated levels of hormones such as FSH, LH, and estradiol. However, even if the test results are normal, findings such as low sperm count ("testicular azoospermia") or testicular atrophy can serve as criteria for diagnosis. Furthermore, in recent years, diagnostic methods using cells inside the mouth (oral epithelial cells) have also become available. In addition to chromosome testing (karyotype analysis), more detailed investigations using genetic tests such as FISH, PCR, and NGS are also possible. In particular, the method of using cells inside the mouth is highly accurate and causes less physical burden, making it helpful for screening Klinefelter syndrome.
Treatment ※4
In the treatment of Klinefelter syndrome, evaluation of social adaptation and psychological support are important. After puberty, male hormone replacement therapy may be performed. In addition, short-term hormone therapy may be conducted from a younger age with the goal of increasing penis size. It is also common to regularly test thyroid function, gonadal function, and bone density. Regarding pregnancy, while it was traditionally considered a cause of infertility in many cases, in recent years, advances in hormone therapy and assisted reproductive technology have increased the cases where natural pregnancy and childbirth are possible. Therefore, if pregnancy is desired, it is recommended to consult a specialist.