Turner Syndrome Detected in Non-Invasive Prenatal Testing
Turner syndrome is a genetic disorder first reported in 1938 by the American physician Henry Turner.
In 1959, the cause was determined to be related to the number of sex chromosomes.
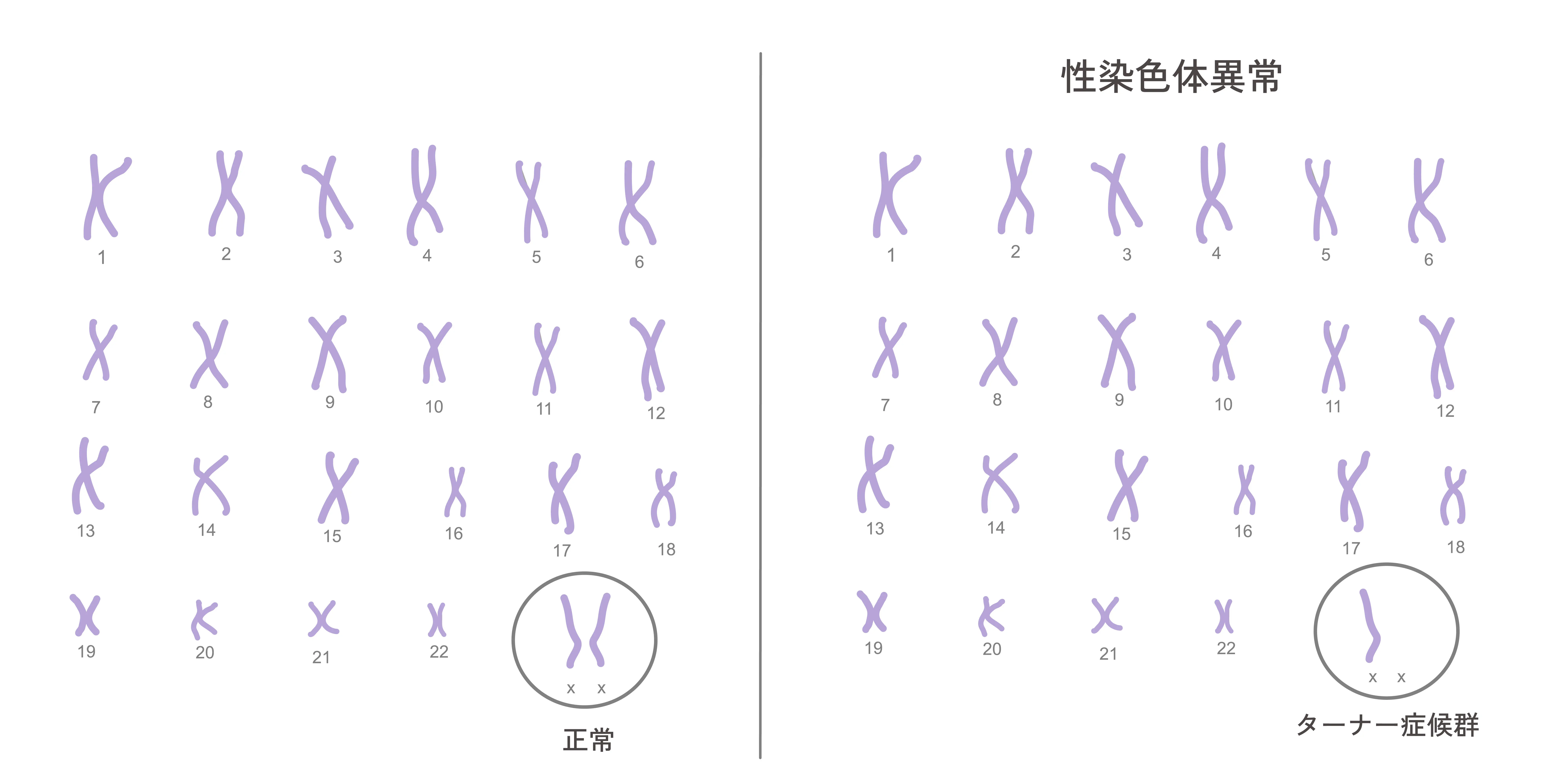
Turner syndrome occurs only in females and is caused by the complete or partial deletion of one X chromosome.
It occurs in 1 out of approximately 2,500 to 3,500 live female births, causing issues such as short stature and adolescent developmental failure.
Identify the Risk of Fetal Turner Syndrome
Non-Invasive Prenatal Testing (NIPT)
Causes
The sex chromosomes that determine human sex are normally XX for females and XY for males, but classical monosomy X (45,X) or structural/partial deletions of the X chromosome can occur. Turner syndrome develops due to these sex chromosome level abnormalities. Although fetuses with Turner syndrome account for about 1.5% of all pregnancies, more than 99% of them result in miscarriage during pregnancy. Only about 0.1% survive to birth.
Turner syndrome is classified into the following 3 types:
1. Classical Monosomy X (45,X)
The most common type, accounting for 40% to 60% of all cases.
2. Partial Monosomy X
Accounts for 20% to 25% of all cases.
The number of chromosomes is normally 46, but structural anomalies or partial deletions are seen in the sex chromosomes. In 4% to 8% of cases, parts of the Y chromosome are present, which increases the risk of developing gonadoblastoma.
3. Mosaicism
A type where multiple karyotypes (such as 45,X, 46,XX, 46,XY, or 47,XXX) coexist in different cells.
Accounts for approximately 15% of cases. The individual may have no subjective symptoms and the family might not notice, representing the mildest form of the syndrome.
Symptoms (Frequency)
Physical Characteristics
- •Short stature (growth delay after age 3, final height averaging around 140 cm)
- •Lymphedema (70%)
- •Triangular face, epicanthal folds, low-set ears, fish-like mouth, high-arched narrow palate (82%), micrognathia
- •Short and webbed neck (80%), low hairline at the back of the neck (80%)
- •Shield-shaped chest (75%), widely spaced nipples (78%)
- •Cubitus valgus / outward-turned elbows (70%)
- •Underdeveloped nails (75%), short fourth metacarpals/metatarsals
- •Multiple pigmented nevi
Medical Complications
- •Sexual Developmental Disorders: Due to ovarian dysgenesis, breast development and menstruation do not occur during puberty.
- •Heart Diseases (20–30%): Coarctation of the aorta (15–30%), valve stenosis/regurgitation (33%), aortic aneurysm, pulmonary artery stenosis
- •Otitis Media (80%): Due to middle ear malformations
- •Venous Vascular Abnormalities
- •Kidney Malformations (33–60%): Unilateral or bilateral renal agenesis, dysplasia, horseshoe kidney, ectopic kidney, duplication
- •Hypothyroidism (10%)
- •Obesity: Weight gain is common due to low metabolic efficiency
- •Diabetes: Type 1 in children, Type 2 in adults or obese individuals
- •Hypertension
- •Osteoporosis: Caused by lack of estrogen
- •Chronic Colitis
- •Intellectual and Emotional Issues: Intelligence is normal, but psychological challenges may arise due to low self-esteem and inferiority complex related to physical characteristics
Diagnostics
When the disorder is suspected due to short stature, delayed puberty, or physical characteristics, peripheral blood chromosome testing was used before NGS (Next-Generation Sequencing) became widely available to collect blood and examine sex chromosome abnormalities.
Even if no abnormalities are found in the peripheral blood chromosomes, retesting using skin cells may be required, and hormone tests are performed as supplementary assessments.
There are three primary diagnostic methods:
1. FISH Method (Fluorescence In Situ Hybridization)
The most standard diagnostic method is chromosome analysis.
Turner syndrome is characterized by the complete deletion or structural anomaly of one X chromosome.
The FISH method uses fluorescent probes to identify specific genes or sequences on the chromosome to detect anomalies.
In Turner syndrome, it is effective in identifying deletions or abnormalities of the X chromosome.
2. PCR Method (Polymerase Chain Reaction)
Symptoms
Testing is conducted using the PCR method, which was commonly used for COVID-19 testing.
Specific regions of the X and Y chromosomes are amplified, enabling diagnosis by verifying the presence of only a single X chromosome without any Y chromosome.
It is particularly effective in checking for specific gene mutations on the X chromosome.
3. Next-Generation Sequencing (NGS)
Symptoms
Overseas, molecular biological testing using DNA analyzers called NGS, commonly used in NIPT, is on the rise. Recently, the number of cases diagnosed via NIPT in Japan has also been increasing.
Alternatively, it is also possible to collect oral mucosal cells from born subjects and analyze the extracted DNA using NGS.
Treatments
Regular hormone therapy is primary, aiming to correct physical abnormalities and manage growth and sexual developmental disorders.
Correction of Physical Abnormalities
Surgery for webbed neck, ptosis, etc.
Growth Disorder Treatment
Growth hormones, anabolic steroids, and estrogen formulations
Sexual Development Treatment
Estrogen therapy to promote development of breasts, uterus, and vagina